The State of the Trans Debate, 2026

Nearly half a decade ago, I wrote an overview1 for this magazine of the debates—and, let’s face it, vicious culture wars—around what’s become known as “gender-affirming care” for youth—psychological and medical interventions based on an internal “gender identity.”
Since then, many revelations about both the research and history of youth gender medicine, and a series of shocking scandals, have emerged. Thus, I assumed that by 2026, many more people, from parents to politicians, would have a deeper understanding of these issues, and that, instead of fighting, we’d be discussing the best, safest, and fairest approach to treating gender dysphoric youth.
Well, you know what they say about assuming. We’re still fighting, and still looking at gender-affirming care through a political lens—rather than through one of ethics and science.
I’m going to recap that original piece here, then go through the significant changes that have taken place since 2022 to explain where we are now—and where we still need to go.
A Brief History
Youth gender medicine—puberty blockers, cross-sex hormones, and sometimes surgeries like double mastectomies or orchiectomy (removal of testicles)—began in the late 1980s in the Netherlands. Doctors found that adults who’d medically transitioned had increased rates of psychological problems—and even completed suicide—after the procedures.2 They surmised that the problem was an inability to “pass” as the opposite sex, especially for natal males. The effects of male puberty, like Adam’s apples and broad brows, were difficult to overcome. Treating children before puberty with what was then called “gender identity disorder,” Dutch clinicians wrote, would lead to “higher percentages of individuals who would more easily pass into the cross sex role” before “the development of secondary characteristics.”3
Youth gender medicine started not because treatment had been successful for adults, but because it hadn’t been. The goal was to pass as the opposite sex, thus alleviating distress about the sexed body. Two Dutch studies, published in the 2010s, suggested that early intervention accomplished these goals.4 The Dutch only treated patients with early-onset gender identity disorder, who lived in supportive families, and whose other mental health problems were attended to. They cautioned against socially transitioning prepubescent kids.
Though some American doctors provided sporadic access to these interventions, they officially arrived here only in 2007, when the first youth gender clinic opened at Boston Children’s Hospital. They were unable to replicate the Dutch approach, for many reasons: lack of socialized medicine, not enough trained psychologists, and an increasingly politicized atmosphere, which derided clinicians evaluating patients, and determining whether or not they could transition, as “gatekeeping.”
American clinicians developed an alternative approach known as “affirmation,” which involved not questioning the young person’s gender identity, and viewed transition as a human right, rather than a psychological and medical intervention. Meanwhile, dozens of new gender identities emerged, from nonbinary to neutrois to bigender. The Obama and Biden administrations both focused heavily on institutionalizing gender identity, prohibiting discrimination based on it, which ultimately led to trans girls and women—that is, natal males—in girls’ and women’s sports and spaces.5 Schools were required to teach about or protect gender identity, in order to retain federal funding—even for school lunches6—and young people with novel gender identities found each other through social media. The number of young people identifying as trans exploded, from 0.6 percent of adults to three times as many youth.7 In Oregon alone, one in 250 girls took testosterone between 2016 and 2023; the state saw a 10-fold increase in girls and 14-fold in boys.8 It was one of the swiftest and most all-encompassing rights movements—and accompanying medical fields—the world has ever seen.
But much of the movement’s rise depended on hiding basic facts—and censoring dissent.
Gender and Sexuality: Birds of a Feather
Despite many advocacy groups asserting that gender and sexuality are separate,9 they’re actually often linked. Many children who suffered from what was, until 2013, called “Gender Identity Disorder” desisted; they stopped feeling dysphoric or wanting to transition, and many grew up to be same-sex attracted.10 That is, there’s a large crossover between early-onset gender dysphoria and later homosexuality.
The claim that transition mitigated suicide risk wasn’t based in fact or science, but was often wielded by advocates to silence critics.
Males who are not feminine and same-sex attracted, and who often experience distress at their sexed bodies or social category later in life, are thought to be “autogynephilic”: attracted to the idea of themselves as women.11 Their distress was also rooted in sexuality, albeit one many people will not admit.
The former category were kids like Jazz Jennings. The latter: adults like Caitlyn Jenner. The ever-widening umbrella of trans flattened them into the same cohort, assuming they needed the same treatment.
Rapid-Onset Gender Dysphoria
In the 2010s, a third cohort of adolescent-onset cases emerged, which a public health doctor and researcher named Lisa Littman described as “rapid-onset gender dysphoria.”12 Unlike with early-onset gender dysphoria—often a precursor to homosexuality—or autogynephilia, ROGD came on suddenly and mostly in girls, many of them suffering from other mental health problems and after sustained social media use. Littman theorized it was a form of “social contagion”—a term that, while technically neutral—offended those fighting for trans rights and increased acceptance. The term was quickly politicized and attacked by most liberal institutions and supporters of gender-affirming care—rather than studied, as it should have been. A new cohort, and new clusters of patients, shouldn’t necessarily access the same treatment as other cohorts, even if they share a diagnosis or a social category like trans.
The Suicide Myth
Proponents of youth gender medicine asserted that it was life-saving. By that, they meant that people under the trans umbrella tend to have higher rates of suicidality than the average population and that social and medical transition would decrease those rates.
Unfortunately, no good evidence supports that claim. Suicidality is generally the result of multiple factors, and even in one of the few follow-up studies conducted in this country in recent years, some patients felt better after transition, while two out of 314 committed suicide after social and medical transition.13 The claim that transition mitigated suicide risk wasn’t based in fact or science, but was often wielded by advocates to silence critics. Even ACLU lawyer Chase Strangio, a trans man, admitted before the Supreme Court that completed suicide “thankfully and admittedly, is rare.”14
Detransitioners
Much of the culture war has centered around detransitioners—those who medically transition and then try to reverse course as much as their bodies can, living as their natal sex. Proponents of youth gender medicine insist detransitioners are rare, and that most detransition for “external” reasons, like stigma, access, or cost.15
The truth is, the rate of detransition is unknown,16 and many people clearly detransition for internal reasons; regret; the realization that gender identity was not the source of their troubles; or internalized homophobia, to name a few.
As there are no billing codes or guidelines for detransition—and Democrats have repeatedly blocked any bills requiring health care for them—detransitioners have enormous trouble getting their medical and psychological needs met.17 We don’t know what percentage detransition, and we also don’t know how to help those that do.
Systematic Reviews and European Retreats
American advocacy groups like GLAAD declared that, about gender-affirming care, “the science is settled.”18 Former Assistant Secretary of Health, Admiral Rachel Levine, called it “suicide prevention” and “well-established medical practice.” Yet by 2022, we knew that neither of those statements was accurate.19
Several European countries had already shifted their approaches toward caution and away from medical intervention. England,20 Finland,21 and Sweden22 had all commissioned systematic evidence reviews (as had the state medical board in Florida)—comprehensive analyses of all available research studies on the topic. They all came to the same conclusion as Sweden’s health board did, that “existing scientific evidence is insufficient for assessing the effects of puberty suppressing and gender-affirming hormone therapy on gender dysphoria, psychosocial health, and quality of life of adolescents with gender dysphoria.”23 That is: the evidence base was so weak that no one could determine if transition carried benefits, while many risks were relatively clear. This applied even to the original Dutch studies, the basis for all youth transition; they actually couldn’t prove any benefit of medical intervention. Thus, per Sweden, pediatric gender treatments were actually “experimental.” In the face of weak evidence, these countries advocated for the least invasive treatment: psychological support.
In response, a Dutch paper questioned why gender-affirming care was required to show benefit at all, dismissing “the expectation that transition should lead to improvement,” as a “normative assumption.”24
Sanctuaries and Bans
In America, there aren’t nonpartisan medical groups. Major U.S. medical organizations—such as the American Medical Association (AMA), American Academy of Pediatrics (AAP), Endocrine Society, and similar groups—are professional associations that engage in advocacy, lobbying, and policy promotion, rather than purely neutral, nonpartisan scientific bodies. In other words, we have advocacy groups that represent the interests of their clinician members. Initially, none of those medical associations shifted, even based on these consistent findings from some of the most liberal countries, with the best health care, in the world. They saw transition more as a human right than a medical issue.
Activists in America and Canada pushed for counseling to understand the source of one’s gender dysphoria to be labeled “conversion therapy.”25 They conflated talking about the source of one’s distress with electroshocking gay people, putting clinicians in the very uncomfortable position of having to protest conversion therapy bans. In 2025, the Supreme Court upheld the right to practice such therapy, but Colorado effectively banned it anyway.26
Furthermore, the U.S. lacks universal healthcare, which makes the government fiscally responsible to its citizens, who would not want their taxes covering treatments with uncertain benefits and certain harms.
So, in the absence of any mechanisms to debate or reform, the issue was subsumed by politics. Beginning in 2021, some Republican-majority states banned gender-affirming care for minors. Beginning in 2022, some Democratic-majority states created “sanctuaries,” which allowed minors from states where interventions were banned to access treatments, in some cases without parental consent.27 We have essentially created a patchwork quilt, mirroring abortion, in which gender-affirming care is banned in some states and legal in others.
WPATH Scandal
In 2022, an advocacy group made up of clinicians and activists, known as the World Professional Association for Transgender Health (WPATH) released its long-awaited eighth “Standards of Care for the Health of Transgender and Gender Diverse People.”28 For the first time, it included a separate chapter on treatment for adolescents, distinct from treating prepubescent children. Though a draft of the document had included an ethics chapter, it was removed from the final version, and a new chapter on “eunuch gender identity” was added.
Despite the completion of several systematic reviews, mentioned above, SOC-8 claimed that a “systematic review regarding outcomes of treatment in adolescents is not possible.” Instead, authors summarized selective studies with positive findings, declaring only that “the data show early medical intervention … can be effective and helpful for many transgender adolescents seeking these treatments.” WPATH claimed they’d crafted the document “based on the best available science and expert professional consensus.”
|
Procedure |
Dutch Protocol (2012) |
Endocrine Society (2017) |
WPATH V7 (2011) |
WPATH V8 (2022) |
|
Social Transition |
Post-Puberty |
Neutral |
No Recommendation |
No Recommendation |
|
Puberty Blockers |
12 |
As soon as puberty begins |
As soon as puberty begins |
As soon as puberty begins |
|
Cross-Sex Hormones |
16 |
16 unless “compelling reasons” |
Age of majority, “in many countries, 16” |
14 |
|
Mastectomy |
18 |
No Recommendation |
1 year of crosssex hormones |
15 |
|
Breast Augmentation |
18 |
Not mentioned |
Not mentioned |
16 |
|
Vaginoplasty, Metoidioplasty, Orchidectomy |
18 |
18 |
Age of majority |
17 |
|
Phalloplasty |
18 |
Not mentioned |
Age of majority |
18 |
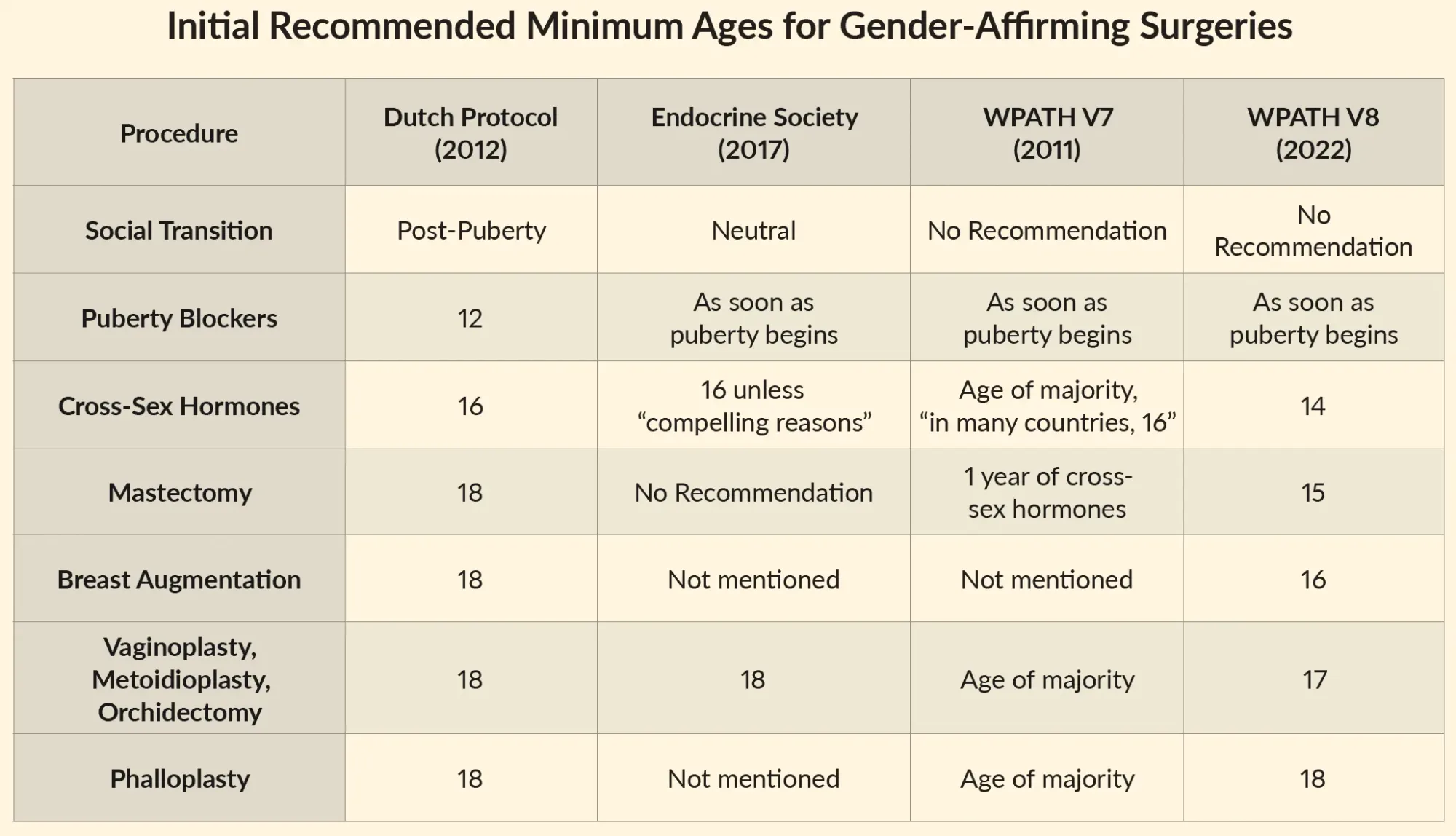
When the new standards first appeared online, they included recommended age minimums for interventions: blockers at whatever age puberty began; 14 for cross-sex hormones; 15 for mastectomy (breast removal); 16 for breast augmentation (creation of breasts); 17 for vaginoplasty (creation of a neo-vagina), metoidioplasty (lengthening of clitoris to resemble a small penis), and orchidectomy (removal of testicles); and 18 for phalloplasty (creation of a phallus). See table above.
The federal government, medical associations, and advocacy groups had conspired to advance their political goal over science.
By the end of the day WPATH published its report, the interventions had disappeared from the document, which WPATH chalked up to a publishing error.
But when advocacy groups like the ACLU sued the states that had banned pediatric gender medicine, amicus briefs and evidence made their way to the Supreme Court.29 We learned what really happened.
WPATH had contracted Johns Hopkins’s Evidence-Based Practice Center to conduct systematic evidence reviews. When they found the same low-quality evidence as the systematic reviews described earlier in this article, WPATH suppressed their publication, allowing only the sharing of data that would be “for the benefit of advancing transgender health in a positive manner.”30 Fearful that age minimums would add fuel to the bans’ fire, the American Academy of Pediatrics and Dr. Rachel Levine, a trans woman who was then the Assistant Secretary of Health, pressured WPATH to remove all age limits for surgeries. The federal government, medical associations, and advocacy groups had conspired to advance their political goal over science.
This enormous scandal warranted little coverage in the press, and didn’t impact the gender medicine industry.
The Cass Review and the American Response—or Lack Thereof
In 2022, England announced the closure of its only national youth gender clinic, Gender Identity Development Service (GIDS) following evidence reviews and investigations into the clinics.31 It didn’t officially shutter until 2024, the year that esteemed British pediatrician Dr. Hilary Cass released an “Independent review of gender identity services for children and young people.”32 The four-year investigation found pediatric gender medicine to be “an area of remarkably weak evidence.” Cass advised that there were many pathways to gender dysphoria, and many pathways out of it; called for an end to specialty gender services; and urged caution for socially transitioning minors, among many other recommendations for reform.
The Cass Review was the most comprehensive work ever crafted on the subject of pediatric gender medicine, but many activist and advocacy groups opposed it, insisting it was politically motivated or methodologically flawed. Initially, the British Medical Association sided with the activists,33 but after conducting its own review34 (yes, it was a review of a review of a review), the BMA largely endorsed Cass’s findings.35
In America, most liberal media outlets and supporters36 of gender-affirming care either ignored the Cass Review or impugned it, rather than wrestling with its findings.
If no benefit could be proven, and harms were known, was gender-affirming care for youth ethical?
WPATH responded that they were “deeply concerned about the facts regarding the Cass Review’s process and content, as well as its consequences for the provision of care for trans and gender diverse youth.”37 They argued that Dr. Cass had no experience working with trans children, when it was her objectivity that qualified her. They asserted that the Review contained no research, but that was the point: to evaluate the research that had been used to justify youth gender medicine, and which, it turned out, didn’t do so. They politicized and denied the science, critiquing the methodology, or asserting that personal experience with trans patients was what mattered. A group of clinicians from Yale, UCSF, and elsewhere, calling themselves “The Integrity Project,” claimed the Cass Review was based on “profound misunderstandings of the evidence base,”38 accusing the Cass Review of repeating “spurious, debunked claims about transgender identity and gender dysphoria.” In particular, they objected to engaging with Littman’s theory of a social contagion and a new cohort of trans youth—not because the demographic changes weren’t clear, but because they found the theory of demographic change offensive. They attacked the studies showing high rates of desistance as outdated, even though the age of the research matters much less than the quality. They argued that puberty blockers should not improve rates of gender dysphoria alone, so that if studies showed they didn’t have benefits, that was fine. In other words, rather than engage with the Cass Review’s recommendations of reinventing gender services for youth so they are more holistic, they argued against there being any problems at all.
The Trump Doctrine
This was the state of youth gender medicine—hopelessly politicized, with supporters unwilling to budge, and Republicans steaming ahead—when, in November 2024, Donald Trump won reelection. His win was partly attributed to his political ads with the tagline “Kamala is for they/them. President Trump is for you.”39 He was capitalizing on the average American’s antipathy toward identity politics, and Democrats’ prizing the needs of a small minority over the majority. Indeed, none of the aforementioned revelations had inspired a shift in rhetoric or policy from the left side of the aisle.
Gender identity is a belief, not a truth—and medicating according to it is a contested intervention, one that seems to make some people feel better, and others feel irrevocably harmed.
From the moment he took office, Trump set about rolling back laws and policies that privileged gender identity above sex. He released executive orders that defined male and female based on body types, not identity. He restored Title IX to refer to sex, not gender identity, undoing both President Obama’s and Biden’s changes. His cabinet removed public funding for gender-affirming care.
To many Democrats and liberals, as well as people beneath the trans umbrella, the changes felt hateful and harsh—a step backward from a world in which gender identity was a legitimate category and way of dividing society. Some of the policy decisions of the Trump administration were indeed overreach, such as banning all trans people from the military. But other changes, such as those relating to medical treatments, what was being taught in school, or policies built on gender identity were responding to the available evidence.40
The HHS Review
The U.S. Department of Health and Human Services (HHS) also commissioned a review of the existing evidence, which resulted in an American version of the Cass Review. “Treatment for Pediatric Gender Dysphoria: Review of Evidence and Best Practices,” written by a politically diverse group of critics of youth gender medicine, included what we’d learned about the evidence base, as well as an important addition—one WPATH had subtracted: a chapter on medical ethics.41
The Review asked if youth gender medical practices were “consistent with widely accepted principles of medical ethics”—especially beneficence (improvement in the patient) and nonmaleficence (avoiding harm). If no benefit could be proven, and harms were known, was gender-affirming care for youth ethical? If doctors were overstating benefits, such as reducing suicidality, and underselling risks, could anyone truly give informed consent?
These were important questions. But because the document had been ordered by the Trump administration, it, too, was perceived as politicized and dismissed by most of the media and medical associations.
ASPS Statement
Despite the systematic evidence reviews, the rising voices of detransitioners, and the retreat in many European countries, most American medical associations refused to budge.
The one exception was the 11,000-member American Society for Plastic Surgeons. After the Cass Review’s 2024 release, the ASPS released a statement that “there is considerable uncertainty as to the long-term efficacy for the use of chest and genital surgical interventions for the treatment of adolescents with gender dysphoria.”42 In 2026, after the HHS Review, ASPS released an official position statement noting that due to the low-quality evidence, ethical considerations, and known harms, “there is insufficient evidence demonstrating a favorable risk-benefit ratio for the pathway of gender-related endocrine and surgical interventions in children and adolescents.” They recommended that no one under 19 transition:
Consistent with ASPS’s August 2024 statement that the overall evidence base for gender-related endocrine and surgical interventions is low certainty, and in light of recent publications reporting very low/low certainty of evidence regarding mental health outcomes, along with emerging concerns about potential long-term harms and the irreversible nature of surgical interventions in a developmentally vulnerable population, ASPS concludes there is insufficient evidence demonstrating a favorable risk-benefit ratio for the pathway of gender-related endocrine and surgical interventions in children and adolescents. ASPS recommends that surgeons delay gender-related breast/chest, genital, and facial surgery until a patient is at least 19 years old.43
Rethinking Gender Identity
Among the most important issues with pediatric gender medicine is what is being treated. If originally transition was to alleviate distress, and make it easier to pass, those goals have largely been discarded in the face of a revolutionary approach to gender identity—not just male and female, but dozens of neo-identities and pronouns like xi and xir to match.
Few proponents have stopped to ask what gender identity is, and to question whether everyone has one. In fact, there are several theories of gender identity.44 One is that it’s simply an awareness of one’s sex—and one would need such an awareness in order to be distressed about it. Another is that it’s a cognitive phase, when toddlers become aware that there are two sex categories, and that they belong to one or the other. They base their sense of what category they belong to on their adherence to gender norms. By around age six or seven, that phase cedes to another: gender constancy, when kids realize their category is based on bodies, not stereotypes.
The third theory is that gender identity is a sense of oneself as man, woman, both, neither, or some other category, completely independent of the body. This theory has prevailed, and remained largely unquestioned—but it needs to be. That is a subjective belief—one anyone is entitled to. But it is not an objective fact, as biological sex is. Still, many young people, including those who’ve gone to medical school, were reared with this version of gender identity as an indisputable reality, and do not understand that it is a political category, not a biological one.
Clinicians, teachers, parents, and patients should be informed of these various competing theories, and not simply taught one of them as a fact.
What Now?
Halfway through 2026, very little has been resolved. Many pediatric gender clinics shuttered in the face of President Trump’s executive orders, but others have sued to stay open or are actively fighting to. In Democratic-majority states, sports and spaces remain divided by gender identity—in Republican-majority states, by sex. Amid chaos and instability in the U.S., it’s hard to have a nuanced conversation about anything, let alone one of the most profoundly divisive issues of this century. Accusations of bigotry are often used against those who argue for a more cautious approach.
In order to come to any kind of resolution, we need to distinguish between subjective and objective truths—as Skeptic founder Michael Shermer puts it, “what is actually true, not just what we want to believe is true.” He writes that “a scientific truth is a claim for which the evidence is so substantial it is rational to offer one’s provisional assent.”45 There is no substantial evidence about gender-affirming care, and its proponents have given unequivocal, not provisional, assent. Gender identity is a belief, not a truth—and medicating according to it is a contested intervention, one that seems to make some people feel better, and others feel irrevocably harmed.
What we can do is continue to calmly state the facts that do exist, and help people understand the complexity of gender-affirming care, outside of politics. Those for it, and those against, almost always have the same goal in mind: the well-being of children.